Meniscal Tears
Hello and welcome back to the ThreeSpires Physiotherapy blog where we take a look at all things physiotherapy and health related. In this blog we are going to look at a particular part of the knee that can get injured and cause problems: the meniscus.
I think when talking about a structure such as the meniscus in the knee it is important to have a good understanding of what the structure is, the anatomy and where it can be found before considering specific injuries and rehab for these injuries. So I think we should now have a look at what the meniscus is.
What is the Meniscus?
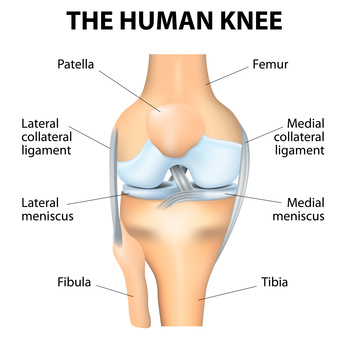 Okay, firstly there are actually two menisci: the lateral meniscus and medial meniscus which are located deep inside the knee joint itself and cannot be felt from the outside. They are a bit of a wonder of biomechanical engineering and have a range of roles which we will look at in more detail later. The menisci are made up of fibrocartilage and are secured to the tibia located upon the tibial plateau – this is the very top of the tibia (shin bone) which runs up to form the knee joint where it meets the femur (thigh bone). They are semi-circular in shape and concave on the top with each end forming a horn which connects to the tibial plateau. It is important to note that the lateral and medial meniscus have some differences between them which are important to understand.
Okay, firstly there are actually two menisci: the lateral meniscus and medial meniscus which are located deep inside the knee joint itself and cannot be felt from the outside. They are a bit of a wonder of biomechanical engineering and have a range of roles which we will look at in more detail later. The menisci are made up of fibrocartilage and are secured to the tibia located upon the tibial plateau – this is the very top of the tibia (shin bone) which runs up to form the knee joint where it meets the femur (thigh bone). They are semi-circular in shape and concave on the top with each end forming a horn which connects to the tibial plateau. It is important to note that the lateral and medial meniscus have some differences between them which are important to understand.
Medial Mensicus
Of the two menisci the medial meniscus is the larger with the rear being broader than the front and it attaches to the tibial plateau just near the anterior cruciate ligament. Fibres from the medial meniscus connect to the transverse ligament of the knee and the outside of the medial meniscus attaches to the joint capsule of the knee .
Lateral Meniscus
The lateral meniscus is slightly smaller than the medial meniscus and forms approximately 4/5 of a circle. There are also several important ligaments which play a key role in securing and connecting the lateral menisci to the knee: the posterior cruciate ligament (PCL) is attached to the lateral meniscus via two ligaments: the ligament of Humphrey and the ligament of Wrisberg. It is important to note that there is anatomical variance here and some people will have both of these ligaments and other people will only have one. As with the medial meniscus the lateral meniscus is also attached to the transverse ligament of the knee.
Blood Supply
Now, going into detail about the blood supply of each of the menisci is certainly beyond the scope of this article but in terms of healing and injuries it is worth considering how vascular the menisci are and why this might impact their healing. Initially after birth menisci have a good blood supply but slowly through childhood this blood supply and vascularisation recedes until eventually in adulthood each meniscus will only have blood supply in the peripheral region and the inner areas will be relatively avascular (lacking blood supply). This in general means that each meniscus can be thought of as having 2 main areas an outer area relatively well supplied with blood and an inner area with minimal blood supply. This impacts the potential for healing of the meniscus in each of these areas, as good blood supply is usually linked with good healing potential. So injuries in the outer area of the menisci (the relatively vascular area) are much more likely to heal well and injuries in the inner area of each menisci (relatively avascular) are less likely to heal and more prone to degeneration.
What is the role of the Mensicus?
The meniscus play a wide range of roles in the knee during standing, jumping, walking and running. The menisci transmit load through the knee joint in a safe manner, offer shock absorption and also aid in the lubrication and nutrition of the articular cartilage of the knee. The wedge shaped nature of the menisci helps secure the femoral condyle (which is curved and bears a resemblance to a knuckle) onto the flat plateau of the tibia. During gait, the menisci are compressed and this ability to be compressed translates vertical force in the knee to horizontal force and offers a method of shock absorption. Research on load in the menisci has shown that they occupy 60% of the contact area between femur and tibia and take approx. 50% of the load. The amount of load that they transmit seems to be very dependent upon knee flexion and at 90 degrees of knee flexion the lateral meniscus is responsible for almost all the load through that lateral compartment of the knee whereas the medial meniscus only takes about half of the load in the medial compartment.
Okay, I think that is probably enough detailed anatomy of the meniscus for now and we shall now look at the symptoms of meniscal tears and meniscal injuries and who is most likely to get them.
What are the Symptoms of a Meniscal Tear?
 In general, the symptoms of a meniscal tear or lesion are fairly easy to define and unlike other knee conditions such as patella-femoral pain will in general be felt deep within the knee and will be accompanied by swelling:
In general, the symptoms of a meniscal tear or lesion are fairly easy to define and unlike other knee conditions such as patella-femoral pain will in general be felt deep within the knee and will be accompanied by swelling:
- Pain, this is very likely to be severe and often the patient will describe a clear mechanism of injury (although this is less likely in older patients). Pain will also be described as being inside the knee rather than on the exterior.
- Swelling: certainly in the early days there may be quite significant swelling and associated loss of range of motion.
- Locking: a “classic” sign of a meniscal injury is a feeling of the knee locking into place and then needing to be twisted slightly to “unlock” it. Although this is the “textbook” sign of a meniscal tear it is not very often present.
An important point to note is that these could be the symptoms of quite a few other conditions and not just a meniscal tear and it is important that you get it confirmed by a professional (such as a physiotherapist) that you actually do have a meniscal tear.
What Causes Meniscal Tears or Injuries?
 Although a simple question the answer to the question: what causes meniscal tears or injuries is complicated by the fact that the underlying causes will be different for a younger age group than it will be for an older age group. The main point to be aware of is that (in general) meniscal tears in a younger (and most likely more sporting) age group are caused by trauma and a twisting and cutting motion, whereas meniscal tears or injuries in an older age group have a degenerative component to them. Where the boundary between ages and between degeneration and trauma lies is a matter of considerable research and argument that we shall try to cover briefly. In general, though, below is a summary of common causes of meniscal tears for all age groups:
Although a simple question the answer to the question: what causes meniscal tears or injuries is complicated by the fact that the underlying causes will be different for a younger age group than it will be for an older age group. The main point to be aware of is that (in general) meniscal tears in a younger (and most likely more sporting) age group are caused by trauma and a twisting and cutting motion, whereas meniscal tears or injuries in an older age group have a degenerative component to them. Where the boundary between ages and between degeneration and trauma lies is a matter of considerable research and argument that we shall try to cover briefly. In general, though, below is a summary of common causes of meniscal tears for all age groups:
Some common causes of Meniscal Tears are:
- A twisting and rotating force at the knee. This will often be in a sporting event such as football, netball or basketball and the player will have landed and be twisting or cutting away with the knee in flexed position. The player will often feel an immediate pain and be unable to continue.
- Trauma: here there is again a very clear mechanism of injury and it may be that the patient has sustained an impact to the knee in a road traffic accident or collision with another player on the field. Again the person involved will almost always report immediate pain and swelling.
- Degeneration: this is often the situation that older patients or players will find themselves in. There will have been no clear cut event or injury that they can remember and they will have just noticed that their knee swells up at times and can with very little cause become painful. Sometimes there will have been an initial event but this is often not a major thing and the knee has always been vulnerable since then.
I think you can see that mainly the causes of meniscal tears break down into two underlying causes. Firstly: a rotational force in a flexed position normally in a sporting event such as football causing a clear tear to an otherwise healthy meniscus and secondly: a generally degenerative (worn out) meniscus that just gives and tears with little cause. There is obviously going to be a certain amount of crossover between these two extremes but clearly a 21 year old who twists their knee playing football and feels an immediate pain is likely to have a different meniscal problem than a 60 year old runner who has been getting intermittent knee pain and swelling for the last few years with no clear cause or potentially has twisted their knee when running and is now experiencing swelling and pain. The difficulty in determining underlying cause and the best course of treatment arises in the groups in between these two and it is often very difficult to be certain of the underlying cause of problems in someone like a 40 year old runner with knee pain after tripping over and twisting the knee.
Who is at Risk of a Meniscal Tear or Injury?
Well, clearly anyone with a knee can have a meniscal injury or tear but there are some factors that make injury more likely.
- Age: the most common age for having a meniscal tear is between 20 – 30 which makes sense as this is a period of life when many people will be very active playing various sports such as football, netball or basketball.
- Male: men are in general much more likely to experience a meniscal tear (possibly 4 x more likely according to some research. The reasons most likely are due to the higher number of males playing sports such as football that require twisting and cutting movements.
 Anyone involved in a sport or activity that involves jumping, landing, turning and twisting at speed. Sports such as football, netball, basketball, hockey and rugby all involve this kind of motion and have a risk of meniscal tears as a result.
Anyone involved in a sport or activity that involves jumping, landing, turning and twisting at speed. Sports such as football, netball, basketball, hockey and rugby all involve this kind of motion and have a risk of meniscal tears as a result.
How is a Meniscal Tear or Injury Diagnosed?
 Usually, at least initially, a meniscal tear will be diagnosed through a combination of symptoms and a physical assessment by a physiotherapist. At this point a variety of factors such as age, sporting background, severity of symptoms, length of symptoms and the patient’s goals will determine whether or not an MRI is required to confirm the diagnosis. Sometimes patients will initially go to their GP with knee pain and then be referred on to a physiotherapist. The physio at this point will take a full history, do a physical assessment and based on the combination of these factors make a diagnosis of a meniscal tear or injury. As with most sporting injuries It is best to get an early diagnosis of a meniscal tear as this allows the best management and treatment plan to be devised and for you to get back to your activity as soon as possible. Delaying a diagnosis and letting things worsen will only lengthen the rehab process needed for your meniscal tear.
Usually, at least initially, a meniscal tear will be diagnosed through a combination of symptoms and a physical assessment by a physiotherapist. At this point a variety of factors such as age, sporting background, severity of symptoms, length of symptoms and the patient’s goals will determine whether or not an MRI is required to confirm the diagnosis. Sometimes patients will initially go to their GP with knee pain and then be referred on to a physiotherapist. The physio at this point will take a full history, do a physical assessment and based on the combination of these factors make a diagnosis of a meniscal tear or injury. As with most sporting injuries It is best to get an early diagnosis of a meniscal tear as this allows the best management and treatment plan to be devised and for you to get back to your activity as soon as possible. Delaying a diagnosis and letting things worsen will only lengthen the rehab process needed for your meniscal tear.
Treatment for Meniscal Tears
Determining the best treatment option for a meniscal tear is not a straightforward matter usually and will depend upon the exact nature of your symptoms and factors such as age, what your goals are, how long your knee has been a problem and how willing you are to have surgery. I think also it is wise to note that things have been changing a great deal over the years in terms of best management of meniscal tears and this is still an area of considerable research. Below I have tried to summarise what the main options/pathways are and when it is most appropriate to use them. The main point to understand is that in thinking about the best treatment for a meniscal tear we are in general trying to decide whether surgery or conservative management (physiotherapy) will be the best option. We will consider the specific exercises that can be used to help with rehab for a meniscal tear but first we need to have a think about who should try physiotherapy and who should consider surgery and any other options.
 Surgery: I know it seems strange that a physio would put surgery as the first option but in this case it is reasonable as the main decision that any physio seeing a patient with a likely meniscal tear or injury needs to make is whether or not surgery would be their best option. So, when would surgery be the best option for a meniscal tear and when should it potentially be avoided and how can we think about these issues and possibly classify patients accordingly? To be clear, as mentioned earlier, this is an area of research where the evidence is not 100% clear but I have tried to combine the evidence with my own experience as a physiotherapist seeing patients with knee pain and meniscal tears.
Surgery: I know it seems strange that a physio would put surgery as the first option but in this case it is reasonable as the main decision that any physio seeing a patient with a likely meniscal tear or injury needs to make is whether or not surgery would be their best option. So, when would surgery be the best option for a meniscal tear and when should it potentially be avoided and how can we think about these issues and possibly classify patients accordingly? To be clear, as mentioned earlier, this is an area of research where the evidence is not 100% clear but I have tried to combine the evidence with my own experience as a physiotherapist seeing patients with knee pain and meniscal tears.
- Degenerative Meniscal Tears: I think it is fair to say that most of the research agrees that if the underlying cause of the meniscal damage is due to degeneration then conservative management and physiotherapy should be the first line of treatment and that this should be a reasonably lengthy period of potentially at least 3 months. In fact, in my opinion we should really extend this out to 6 months so as to give patients a really good chance of making a recovery and getting a functional knee back without the difficulties and risk of surgery. So, who is most likely to have a degenerative meniscus and how might it present. In general these patients will be older (definitely 40+) and quite often they will have had a grumbling knee for some time. The knee pain will sometimes become quite intense and swell up with very little warning. They can sometimes pin point a particular action such as playing football and their knee getting twisted but often they will have no clear mechanism of injury. From my own perspective as a physiotherapist assessing anyone with knee pain like this I will be immediately considering that they may well have a degenerative meniscus that has torn due to wear and tear and that at the very least they need to try exercises and strengthening for a significant period before seeking a surgical opinion.
- Traumatic Mensical Tears: here we have a fairly clear cut case of surgery (or at least a surgical opinion) being the best option. In this case the meniscus has been torn in the peripheral vascular zone and the patient has a classic bucket handle tear of the meniscus. I think most of the research suggests that surgery is most likely to be the best option in this case as the patient has torn their meniscus due to trauma and the meniscus was otherwise generally healthy. Also tears in the outer zone have good blood supply and should heal well. Okay, who is most likely to have this kind of meniscal damage and how will they present? Mostly they will be relatively young (under 30) and they will be able to pinpoint a clear mechanism of trauma such as playing in a football game, twisting and feeling immediate pain deep inside the knee that stopped them playing. The knee is very painful and they are really struggling to see any improvement and if they move it in certain directions it swells up. In this case as a physiotherapist I think it is fairly clear that after most likely the patient needs imaging and a surgical opinion.
- A Mixed Picture: so, the two cases above I think are fairly easy to understand and fairly easy for both patients and physiotherapists to manage. The difficulty comes when we have a bit of a mixed picture and the patient is of an intermediate age let’s say somewhere between 35 and 50. In this case there has been trauma or the patient describes some quite classic signs of meniscal pathology such as locking or swelling after twisting and flexion. Clearly the patient’s knee is likely to have some degeneration (they are not young but nor are they old) and they are quite fit and active. The difficulty they have is associated with keeping fit and doing sport, in normal life they get minimal problems from their knee. I think here it is reasonable to assume that although they have probably have a traumatic meniscal tear and may even have a classic tear of the vascular zone such as a bucket handle tear they are also likely to have some degeneration associated with age. The difficulty arises in determining how much can be associated with degeneration. Here I think it is reasonable to give this patient a fair bit of time with exercises and strengthening to see if they can get a knee that is able to cope with the demands of their sport. At some point though if there is no change they will clearly need a surgical opinion.
- Physiotherapy, Exercises & Strengthening: so, given the discussion above about classification of meniscal tears and who might be needing to see a surgeon we need to have a think about when physiotherapy, exercises and strengthening will be the best approach. We shall start with the category of patients who it seems fairly clear cut that strengthening and physiotherapy will be best for and then progress to more difficult case.
 Older patients with a degenerative meniscus: okay, first point to note is that in general as a physio I try to avoid pigeon holing patients into age categories and ignoring their fitness and lifestyles. Certainly some 70 year old patients that I see are very fit and strong indeed. However, this is one of those situations where age really is an issue in term of what is likely to be the underlying cause of the meniscal damage and the likely success from surgery. I generally think that anyone over the age of 60 with knee pain consistent with a meniscal tear is going to be much better served by physiotherapy and strengthening rather than surgery – at least in the medium term. At the very least patients in this general category really need to have had a lengthy period of rehab and strengthening over at least 8 – 12 months before considering surgery. I can understand how frustrating anyone in this age group with knee pain might find this but I think the evidence is fairly strong here that surgery should be the last resort due to the underlying condition of the meniscus and also in my experience many patients will simply have not tried hard enough on strengthening. Often patients will describe a lengthy period of rehab but on testing it is clear that they have many weaknesses that need addressing first to see if these improve their knee pain.
Older patients with a degenerative meniscus: okay, first point to note is that in general as a physio I try to avoid pigeon holing patients into age categories and ignoring their fitness and lifestyles. Certainly some 70 year old patients that I see are very fit and strong indeed. However, this is one of those situations where age really is an issue in term of what is likely to be the underlying cause of the meniscal damage and the likely success from surgery. I generally think that anyone over the age of 60 with knee pain consistent with a meniscal tear is going to be much better served by physiotherapy and strengthening rather than surgery – at least in the medium term. At the very least patients in this general category really need to have had a lengthy period of rehab and strengthening over at least 8 – 12 months before considering surgery. I can understand how frustrating anyone in this age group with knee pain might find this but I think the evidence is fairly strong here that surgery should be the last resort due to the underlying condition of the meniscus and also in my experience many patients will simply have not tried hard enough on strengthening. Often patients will describe a lengthy period of rehab but on testing it is clear that they have many weaknesses that need addressing first to see if these improve their knee pain. Patients of middle age who are happy to change sports or modify activities: in general these patients will be over 40 and have clear signs of meniscal damage and often will have been doing a particular sport such as football and will have a clear mechanism of injury and trauma. They have tried some rehab but not much and have generally tried to rest their knee and then return to their sport but they have been unable to consistently cope with their sport and have had several re-occurrences of their knee pain. Here the patient is happy to accept that they can’t do that sport to the same level but wants to keep fit and is happy to avoid things that might flare their knee. So, as a physiotherapist I think this is a fairly clear case of someone for whom physiotherapy will be the best approach for a good period of time (potentially at least 6 months) so that they can work on strengthening and stabilising their knee and leg and find out if they can get their knee to the point where they can keep fit and avoid surgery. In my experience once these patients strengthen their knee and avoid the main issues that flare things such as cutting and twisting activities they do very well and are able to avoid any surgery. Often, they will have clear weaknesses in terms of balance and strength that can be addressed that really improve things for them.
Patients of middle age who are happy to change sports or modify activities: in general these patients will be over 40 and have clear signs of meniscal damage and often will have been doing a particular sport such as football and will have a clear mechanism of injury and trauma. They have tried some rehab but not much and have generally tried to rest their knee and then return to their sport but they have been unable to consistently cope with their sport and have had several re-occurrences of their knee pain. Here the patient is happy to accept that they can’t do that sport to the same level but wants to keep fit and is happy to avoid things that might flare their knee. So, as a physiotherapist I think this is a fairly clear case of someone for whom physiotherapy will be the best approach for a good period of time (potentially at least 6 months) so that they can work on strengthening and stabilising their knee and leg and find out if they can get their knee to the point where they can keep fit and avoid surgery. In my experience once these patients strengthen their knee and avoid the main issues that flare things such as cutting and twisting activities they do very well and are able to avoid any surgery. Often, they will have clear weaknesses in terms of balance and strength that can be addressed that really improve things for them.- Very fit middle age patients in high level sport: undoubtedly this category is the most difficult to be certain of the best strategy and the research is not conclusive on the best options. This as a physio makes it very difficult to know the best management strategy for these patients and often it will come down to a discussion with them about their goals and what they are willing to risk. In this case we most likely have a patient over 40 who is fit and strong and who has been continuing with sport at a fairly high level such as hockey at masters level and experienced pain in their knee from twisting and cutting and they wish to return to their sport as soon as possible. They are not willing to stop and want to know what is the best option for them in terms of retuning to playing hockey. So, here we have a difficult case in knowing what is the best option for this person in terms of how long to work on rehab before considering a surgical opinion for their meniscal damage. I think initially at least a period of rehab should be the first option if tolerated as it is often the case that even with these patients they will have weaknesses that can be addressed and that can improve outcome. However, I think it is important for these patients to consider a surgical opinion much sooner than one would usually with this age group. My own approach here is that it is best to have a frank discussion about options and the goals of the patient, this discussion (combined with physical testing) will often make the best treatment option obvious as some patients will immediately want a surgical opinion and others will be very reluctant to consider surgery.
Okay, I think we have looked at enough possible options here, the main thing that I have wanted to convey in this blog is that a meniscal tear is a challenging injury to be certain of what is the best strategy to deal with it. Often, the best strategy will depend upon a combination of age, type of injury, the goals of the patient and response to rehab and strengthening. Next I think we should look at how we might be able specifically to help with a meniscal injury.
How Can ThreeSpires Physiotherapy Help with My Meniscal Tear?
Physiotherapy is extremely helpful if you have injured your meniscus and one of our physiotherapists who is experienced with managing and treating meniscal tears will be able to help. We can help in a number of ways:
- Assessment & Diagnosis of a Meniscal Tear: this as mentioned earlier is a vital part of managing your meniscal injury and the sooner you have an assessment the sooner you will know what you are dealing with. Our physiotherapists will be able to comprehensively assess your knee, make a diagnosis and also identify underlying biomechanical causes of your meniscal tear such as core weakness.
- Management Plan: once a diagnosis of a meniscal injury has been made it is vital that you get a clear and comprehensive plan to optimise your recovery. Your physiotherapist will be able to identify the best strategy for helping with your meniscal injury and will be able to advise on whether or not physiotherapy or a surgical opinion will be the best option.
- Exercises for Meniscal Tears: your physiotherapist will be able to determine which are the most appropriate exercises to help strengthen your knee and improve your ability to cope with your injured meniscus.
- Treatment for Meniscal Tears: In conjunction with load management and exercises your physio will be able to use soft tissue and hands on techniques to treat any areas of your legs that have become overloaded and tight.
- Supplementary Exercises for Meniscal Tears: as part of your assessment for a meniscal tear your physiotherapist will also look at strength and biomechanics in your legs and see if there are any imbalances or weaknesses that might be contributing towards your meniscus getting overloaded. As such they will likely prescribe a series of other exercises designed to improve strength and control and help you cope better with a meniscal injury.
Okay, I hope that you have found this article about meniscal tears helpful. Should you or anyone you know have a meniscal injury or suspect that you have one please get in touch and one of our physios would be happy to help.
REQUEST A CALLBACK
Just fill in the form below and give us a quick idea of your problem/request so that we can be better prepared to help you.